Notes from paper:
Consensus statement on concussion in sport – the 5th international conference on concussion in sport held in Berlin, Oct 2016
McCrory P, et al. Br J Sports Med. 2018;51:838-47.
Individual management of sport related concussion (SRC) and return-to-play decisions remain in the realm of clinical judgement
Recognize
SRC represents the immediate and transient symptoms of TBI
SRC can be caused by a direct blow, or other blow on the body that results in an impulsive force transmission to the head
Rapid onset of short-lived impairment of neurological function that often resolves spontaneously, however, in some cases signs and symptoms evolve in minutes to hours
Symptoms largely reflect a functional disturbance rather than a structural injury, therefore no abnormality is typically seen on standard structural neuroimaging studies
SRC results in a range of clinical signs and symptoms
Sideline Evaluation
In all suspected cases of concussion, the individual should be removed from play and assessed by a physician or licensed healthcare provider
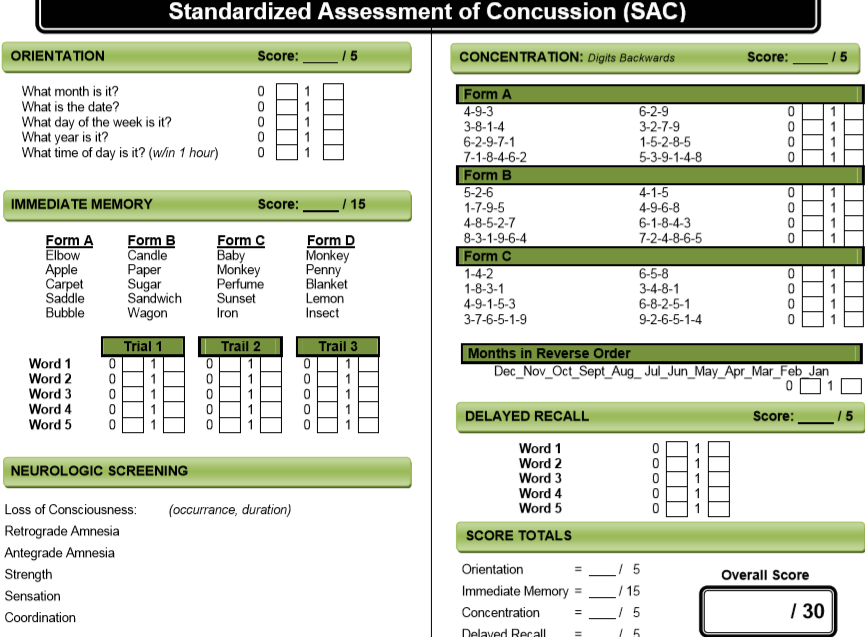
Sideline evaluation of cognitive function is essential. SCAT5, SAC (standardized assessment of concussion)
With clear signs of SRC (LOC, tonic posturing, balance disturbance) immediately removed from participation.
If SRC is suspected, perform assessment tool
If physician has performed assessment and concussion is no longer suspected, the physician can determine the disposition and timing of return to play.
Assessment tools:
Postural stability testing
GCS: Eye opening (4) spontaneous, speech, pain, none. Verbal (5) oriented, confused, inappropriate words, incomprehensible, none. Motor (6) obeys, localizes pain, withdrawal, abnormal flexion to pain, extension to pain, none.
SCAT5 onfield assessment includes GCS, observable signs, memory assessment, cervical spine assessment (age 13 and above)
SCAT5: https://bjsm.bmj.com/content/bjsports/early/2017/04/26/bjsports-2017-097506SCAT5.full.pdf
Child SCAT5 includes GCS, observable signs, and cervical spine assessment
Child SCAT5: https://bjsm.bmj.com/content/bjsports/early/2017/04/26/bjsports-2017-097492childscat5.full.pdf
Standardised Assessment of Concussion (SAC): total score of 30. Injured players score below baseline immediately after injury
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC155418/
With evolving symptoms must consider removal and serial evaluation
SCAT is useful immediately after injury and is the most well-established and rigorously developed instrument available for sideline assessment.
Diagnosis of SRC can be suspected with one or more of the following:
Symptoms: somatic (headache), cognitive (feeling like in a fog), emotional (lability)
Physical signs (LOC, amnesia, neurological deficit)
Balance impairment
Behavioral changes (irritability)
Cognitive impairment (slowed reaction)
Sleep/wake disturbance
Remove player when showing signs or symptoms of SRC until he/she can be evaluated by a physician
When SRC is diagnosed, player should not return to play on the day of injury
The final determination regarding SRC diagnosis and/or fitness to play is a medical decision based on clinical judgement.
Re-evaluate
On follow-up exam perform comprehensive history and detailed neurological examination (MS, cognitive functioning, sleep/wake disturbance, ocular function, vestibular function, gait, and balance)
Improvement or deterioration of signs/symptoms (may also require asking parents, coaches, teammates, etc.
Determination of need for emergent neuroimaging
Rest
Many consensus statements recommend that athletes should rest until they become symptom free.
Statement from this paper: insufficient evidence is present supporting that prescribing complete rest achieves its objectives. After a brief rest in the acute phase (24-48 hrs), encourage patient to become gradually and progressively more active while staying below cognitive and physical symptom exacerbation thresholds (ie activity should not worsen symptoms). Avoid vigorous exertion while recovering.
Rehabilitation
Most individuals recover in 10-14 days.
Data support interventions including psychological, cervical, and vestibular rehabilitation.
Active rehabilitation programs may be of benefit
Graduated return-to-sport (RTS) strategy (table 1 from paper)
| Stage | Aim | Activity | Goal of each step |
| 1 | Symptom-limited activity | Daily activities that do not provoke symptoms | Gradual reintroduction of work/school activities |
| 2 | Light aerobic exercise | Walking or stationary cycling at slow to medium pace. No resistance training | Increase heart rate |
| 3 | Sport-specific exercise | Running or skating drills. No head impact activities | Add movement |
| 4 | Non-contact training drills | Harder training drills, eg, passing drills. May start progressive resistance training | Exercise, coordination and increased thinking |
| 5 | Full contact practice | Following medical clearance, participate in normal training activities | Restore confidence and assess functional skills by coaching staff |
| 6 | Return to sport | Normal game play |
Refer
The term ‘persistent symptoms’ refers to symptoms that persist beyond expected time frames (>10-14 days in adults, >4 weeks in children)
When symptoms persist, a detailed multimodal clinical assessment is required to identify specific primary and secondary pathologies that may be contributing to persisting post-traumatic symptoms.
Treatment should be individualized. Some evidence supports symptom-limited aerobic exercise programs; a targeted physical therapy program (with c-spine or vestibular dysfunction); and/or a collaborative approach including cognitive behavioral therapy.
Limited evidence supports pharmacotherapy. Concussed athletes should not only be free from concussion-related symptoms, but also not taking any medications that may mask or modify symptoms of SRC prior to return to sport.
Recovery
Clinical recovery is defined as a return to normal activities, including school, work, and sport. This encompasses a resolution of post-concussion-related symptoms.
The strongest and most consistent predictor of slower recovery from SRC is severity of a person’s initial symptoms.
Some evidence suggests the high-school years are the most vulnerable time period for having persistent symptoms.
Return to sport
See table above.
If any concussion symptoms occur during stepwise recovery, athlete should drop back to the previous asymptomatic level and progress again after a 24 hr period of symptom free at the lower level.
Reconsider
Temporary absence from school may be necessary after SRC
Should not return to sport until successful return to school.
Residual effects and sequelae
Potential for long-term problems such as cognitive impairment, depression, chronic traumatic encephalopathy (CTE).
Risk reduction
Helmet use in skiing/snowboarding.
Disallowing body checking in youth ice hockey (under age 13)
Limiting contact in youth football practices (although no evidence to support the translation of this reduced contact to reduction in SRC) Tackle training without helmets and shoulder pads do not lead to a reduction in SRC risk.